Piriformis Syndrome Part III- Treatment
Piriformis Syndrome Treatment
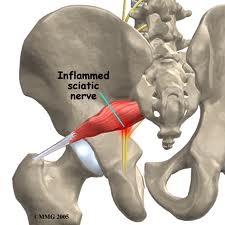
The two main goals of treatment are 1) to relief irritation to the sciatic nerve and 2) address any functional problems that may be contributing.
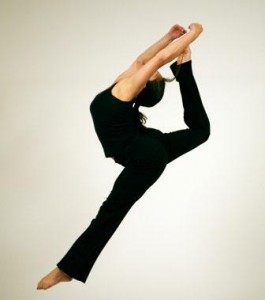
If the sciatic nerve is inflamed the first step is to decrease aggravation from compression. Things to avoid are leg crossing, sitting on your wallet, and sitting on hard surfaces. Things you should begin doing are applying ice to the piriformis, stretching of the piriformi, and taking oral anti-inflammatories (as directed). Stretching every 2-3 hours (while awake) is a key to the success of non-operative treatment. Prolonged stretching of the piriformis muscle is accomplished in while lying on your back with the hip flexed and passively adducted/internally rotated (see picture). Another exercise that can be helpful to decrease irritation between the piriformis and sciatic nerve is a nerve gliding exercise. This exercise tensions the sciatic nerve and allows it to move relative to the piriformis. It is sometimes called nerve flossing to better describe how the nerve moves through other structures. Two types of nerve gliding exercises are pictured below. (Pictures from http://www.dynamicchiropractic.com/mpacms/dc/article.php?id=53203)


Manual therapy can be extremely helpful in releasing tension on the sciatic nerve and addressing functional deficits. Soft tissue therapies, including myofascial release and Graston®, aimed at releasing tension and muscular adhesions within the piriformis can be beneficial. Chiropractic spinal adjustments can help address functional contributions from the spine such as sacroiliac joint hypomobility and low back dysfunction. Hyperpronation of the foot can be addressed through orthotics in the short term and foot strengthening in the long term. Pronation is a normal foot motion however overpronation may lead to increased external rotation of the hip with walking putting tension on the piriformis and sciatic nerve.
Treatment may take several months of consistent work and it is important not to get discouraged. As long as there is no progression of neurological symptoms conservative treatment is the best option. Your symptoms should be monitored by a healthcare practitioner to ensure there is no progression.
-Dr. Kevin Rose, DC






")